



Back to overview – Information
The Structure of the Spine
(Dr.H.Hiertz)
Strictly speaking, we distinguish between 2 organs: I – the spine and the II – nervous system running through it. The discussion takes place separately, but in the clinical assessment both organs must of course always be assessed in order to be able to draw up a concrete therapy plan.
I : Spine
With the exception of the 1st and 2nd cervical vertebrae, the spine has the same structure in the entire area from the cervical to the lumbar spine.
We differentiate between the flexible cervical spine with 7 vertebrae, the relatively immobile thoracic spine with 12 vertebrae and the lumbar spine, which in turn is well flexible, with mostly 5 vertebrae.
The spinal cord usually extends to the 12th / 1st breast. Lumbar vertebrae, only the individual nerves run further downwards – paraplegia is not possible if the lower lumbar spine is diagnosed!
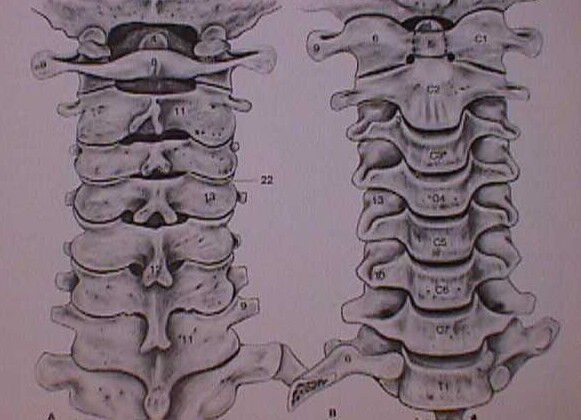
Cervical spine:
Cervical spine from the front. Cervical spine from behind
Cross-section through WS, spinal canal with spinal cord, vertebral joint, vertebral body, emerging nerve, intervertebral disc

The 1st cervical vertebra (atlas) is in articulated connection with the head, actually consists only of the vertebral arches, downward joint to the 2nd cervical vertebra (axis). At the rear edge of the anterior atlas arch is the extension of the 2nd cervical vertebra (dens), which is held in position with ligaments and primarily enables the head to move and rotate. Downward there is an intervertebral disc at the front and a joint to the third cervical vertebra at the back.
From the 3rd cervical vertebra, the structure is the same up to the last lumbar vertebra:
 |  | Spinal canal with spinal cord, vertebral joint, vertebral body, emergent nerve |
678/5000In front is the intervertebral disc and the vertebral body, to the rear comes the bony vertebral canal in which the spinal cord pulls downwards. As can be seen in the picture, the spinal cord only needs part of the canal, the rest is filled with protective layers – spinal fluid, adipose tissue and venous plexus. The nerve emerges from the spine below the intervertebral disc. On the side we have the transverse process, in which the posterior carotid artery (vertebral artery) runs from the 1st to the 6th cervical vertebra. To the rear the limitation with the posterior vertebral arch and the spinous process, which can be felt through the skin at the back, as well as the vertebral joint between the two vertebrae.
The two neighboring vertebrae, the intervertebral disc in between and the vertebral joint at the back, which controls the extent of movement, are referred to as the movement unit or vertebral segment.
Thoracic spine:
Structure exactly the same as from the 3rd to 7th cervical vertebrae

In front are the vertebral bodies, in between the intervertebral discs, to the rear the vertebral canal in which the spinal cord runs, to the side the intervertebral holes where the nerve leaves the spine, to the rear and side the transverse and spinous processes. Relatively immobile due to the bony connection with the chest.
Lumbar spine
The lumbar spine has significantly larger vertebral bodies as the body weight has to be supported. The structure is the same as in the thoracic spine, but only the nerve fibers run in the spinal canal, no spinal cord.
 |  | Vertebral body vertebral joint intervertebral disc spinal canal with nerve fibers |
82/5000The intervertebral discs are of course much larger than in the neck and chest area.
Spine stability
132/5000The stability of the spine is always important in the assessment. You can compare the spine with a crane.
The crane column corresponds to the vertebral bodies and intervertebral discs. Around 80% of the forces acting on the spine are absorbed through this area. If the vertebral bodies or high intervertebral discs are weakened, the crane and the spinal column buckle – a buckling occurs – kyphosis.
If the rear section is weakened by the crane – the vertebral joints, ligaments and muscles on the spine, the tension belt is disturbed and the system shifts. Vertebral displacements occur on the spine – Listhesis, scoliosis.
Curvatures of the spine
Furthermore, the spine has typical curvatures:
In the cervical and lumbar spine there is a forward curvature – lordosis, in the thoracic spine backwards – kyphosis.

441/5000The curvatures are decisive for the harmonious transmission of force in the spine, if these curvatures are correct, there is a vertical line from the 7th cervical vertebra down over the sacrum, at least behind the femoral heads. This curvature is constant from birth and is calculated by measuring the angle from the femoral head to the cross area. We have 4 groups – the larger the angle, the more degrees of lordosis we need.

Knowing these degrees is essential to enable proper surgical planning. If the lordosis level is too flat, we try to compensate for it with the hip and knee joints, which not only causes pain, but also an unsteady gait and an increasingly bent gait pattern. In the case of an operation, the appropriate corrections must then be carried out in order to obtain a good result.
II. Nervous system – cervical / thoracic spine
The spinal cord runs in the vertebral canal in the area of the cervical and thoracic spine. The spinal cord, as it is the most sensitive organ, must be strongly protected against the effects of violence. This happens on the one hand through the bony vertebral canal within the spine, on the other hand through the liquor fluid around the spinal cord within the envelope and outside to the bone through fatty tissue and the venous plexus.
This is also the reason that the spinal cord as an organ only fills part of the spinal canal, the rest is available for the securing spaces. The nerve emerges laterally from the spine, which on the one hand pulls to the corresponding muscle (failure leads to muscle paralysis), and on the other hand carries the information from the periphery to the nervous system. (Failure leads to emotional disorder)
 .. .. Adipose tissue and veins … .. Nerve roots … .. Spinal fluid … .. Spinal cord .. .. Adipose tissue and veins … .. Nerve roots … .. Spinal fluid … .. Spinal cord |
Each nerve has a typical area of spread on the skin and muscle groups that are supplied. In this way, after a closer examination, based on the radiation of pain and deficits (sensory-sensory disturbance or motor-reduced strength), one can clearly determine the height of the spine that is damaged.
 … ..Pressure on the spinal cord … ..Pressure on the spinal cord… ..pressure on the nerve |
In the case of problems with the spinal cord, there may initially be discrete symptoms with coordination disorders in the arms and legs, sensory disorders and the feeling of “like walking on cotton wool”, which can lead to paraplegia. The severity of the severity varies, the level of damage also depends on the losses, up to the high cross-section with paralysis of the arms / legs and breathing.
Every pressure effect can acutely lead to these problems, but it can also chronically lead to organ damage due to the pressure on the organ, the resulting circulatory disorders and the fixation of the myelon – scars develop in the organ that we call myelopathy.
II. Nervous System– Lumbar Spine
In the lumbar spine only the nerve fibers pulling downwards run, the spinal cord hears about at the level of the 12th chest / 1st Lumbar vertebrae open (variable).
 … ..Exciting nerve… ..cauda fibers … ..Exciting nerve… ..cauda fibers |
Only the individual nerve fibers (caudal fibers) run in the spinal canal.
Every nerve has an associated area of spread – from the radiation of pain to sensory disturbances to motor failure (paralysis). The centrally running nerves supply the bladder / intestinal and sexual organs. Failure can lead to partial paralysis in the leg, in extreme cases paralysis of the bladder and bowel function and impotence. Paraplegia is not possible in the lower lumbar spine!